ZYNYZ® dosing and administration1
The recommended dosage of ZYNYZ is 500 mg IV over 30 minutes, every 4 weeks

ZYNYZ COMBINATION THERAPY
Administration in combination with carboplatin and paclitaxel for the first-line treatment of adult patients with inoperable locally recurrent or metastatic squamous cell carcinoma of the anal canal (SCAC).1
Treatment with ZYNYZ should continue until disease progression, unacceptable toxicity, or up to 1 year.1
In the POD1UM-303 study, patients received carboplatin (AUC 5) on day 1 and paclitaxel (80 mg/m²) on days 1, 8, and 15. Refer to the Prescribing Information for the agents administered in combination with ZYNYZ for recommended dosing information, as appropriate.
ZYNYZ MONOTHERAPY
Administration as a single agent for the treatment of adult patients with locally recurrent or metastatic SCAC with disease progression on or intolerance to platinum-based chemotherapy.1
Treatment should continue until disease progression, unacceptable toxicity, or up to 2 years.1
Get more information
on dosing and administration
No dose reduction of ZYNYZ for adverse reactions is recommended1
- In general, withhold ZYNYZ for severe (Grade 3) immune-mediated adverse reactions
- Permanently discontinue ZYNYZ for:
- life-threatening (Grade 4) immune-mediated adverse reactions,
- recurrent severe (Grade 3) immune-mediated reactions that require systemic immunosuppressive treatment, or
- an inability to reduce corticosteroid dose to 10 mg or less of prednisone equivalent per day within 12 weeks of initiating steroids
- Dosage modifications for ZYNYZ for adverse reactions that require management different from these general guidelines are summarized below
Dosage modifications for adverse reactions1
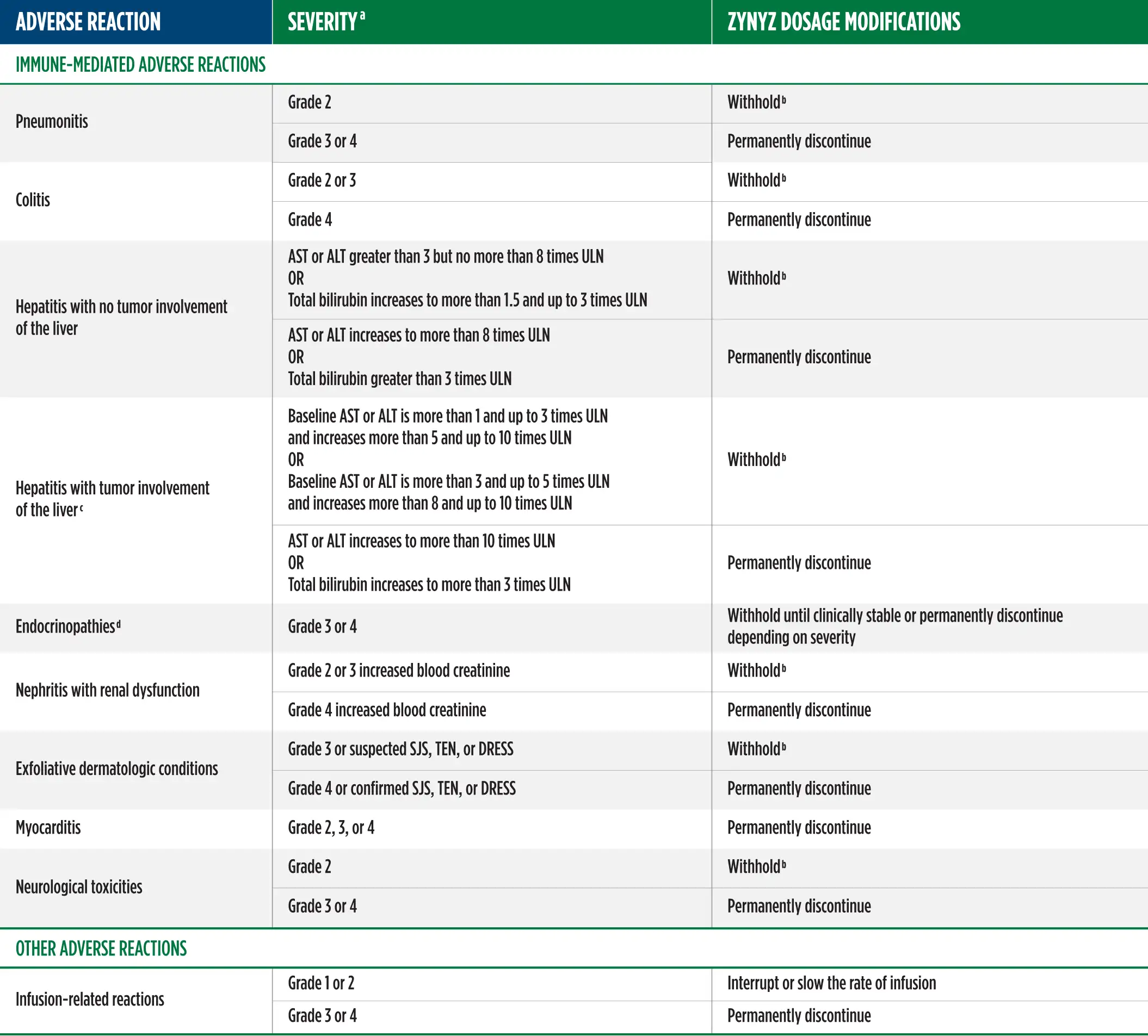
a Toxicity graded per National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) v5.0.
b Resume in patients with complete or partial resolution (Grade 0 to 1) after corticosteroid taper. Permanently discontinue if no resolution within 12 weeks of initiating steroids or inability to reduce prednisone to less than 10 mg/day (or equivalent) within 12 weeks of initiating steroids.
c If AST and ALT are less than or equal to ULN at baseline in patients with liver involvement, withhold or permanently discontinue ZYNYZ based on recommendations for hepatitis with no liver involvement.
d Depending on clinical severity, consider withholding for Grade 2 endocrinopathy until symptom improvement with hormone replacement. Resume once acute symptoms have resolved.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DRESS, drug rash with eosinophilia and systemic symptoms; SJS, Stevens-Johnson syndrome; TEN, toxic epidermal necrolysis; ULN, upper limit of normal.
aToxicity graded per National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) v5.0.
bResume in patients with complete or partial resolution (Grade 0 to 1) after corticosteroid taper. Permanently discontinue if no resolution within 12 weeks of initiating steroids or inability to reduce prednisone to less than 10 mg/day (or equivalent) within 12 weeks of initiating steroids.
cIf AST and ALT are less than or equal to ULN at baseline in patients with liver involvement, withhold or permanently discontinue ZYNYZ based on recommendations for hepatitis with no liver involvement.
dDepending on clinical severity, consider withholding for Grade 2 endocrinopathy until symptom improvement with hormone replacement. Resume once acute symptoms have resolved.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DRESS, drug rash with eosinophilia and systemic symptoms; SJS, Stevens-Johnson syndrome; TEN, toxic epidermal necrolysis; ULN, upper limit of normal.
How ZYNYZ is supplied, stored, prepared, and administered1
Visually inspect the vial for particulate matter and discoloration prior to administration. ZYNYZ is a clear to slightly opalescent, colorless to pale yellow solution and is free of particles. Discard the vial if the solution is cloudy, discolored, or contains particulate matter.
1.
Withdraw 20 mL (500 mg) of ZYNYZ from one vial and discard vial with any unused portion.
3.
Mix diluted solution by gentle inversion. Do not shake.
2.
Dilute ZYNYZ with either 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to a final concentration between 1.4 mg/mL to 10 mg/mL. Use polyvinylchloride (PVC) and di-2-ethylhexyl phthalate (DEHP), polyolefin copolymer, polyolefin with polyamide, or ethylene vinyl acetate infusion bags.
4.
Visually inspect the infusion bag for particulate matter and discoloration prior to administration. Discard if the solution is discolored or contains particulate matter.
Storage of diluted ZYNYZ solution
Protect the diluted ZYNYZ solution from light during storage.
Store diluted ZYNYZ solution:
At room temperature (up to 25°C [77°F]) for no more than 8 hours from the time of preparation to the end of the infusion.
Under refrigeration at 2°C to 8°C (36°F to 46°F) for no more than 24 hours from the time of preparation to the end of the infusion. If refrigerated, allow the diluted solution to come to room temperature prior to administration. The diluted solution must be administered within 4 hours (including infusion time) once it is removed from the refrigerator. Do not freeze or shake diluted solution.
DO
- Administer diluted ZYNYZ solution by IV infusion over 30 minutes
- Use a polyethylene, polyurethane, or PVC with DEHP intravenous line containing a sterile, non-pyrogenic, low-protein binding polyethersulfone, polyvinylidene fluoride, or cellulose acetate 0.2 micron to 5 micron in-line or add-on filter or 15 micron mesh in-line or add-on filter
DO NOT
- Do not co-administer other drugs through the same infusion line
- Do not administer ZYNYZ as an intravenous push or bolus injection
How ZYNYZ is supplied, stored, prepared, and administered1
Supplied in a carton containing 1 single-dose vial of 500 mg/20 mL (25 mg/mL) (NDC 50881-006-03).
- ZYNYZ injection is a clear to slightly opalescent, colorless to pale yellow solution
- Store refrigerated at 2°C to 8°C (36°F to 46°F) in the original carton to protect from light. Do not freeze or shake
Visually inspect the vial for particulate matter and discoloration prior to administration. ZYNYZ is a clear to slightly opalescent, colorless to pale yellow solution and is free of particles. Discard the vial if the solution is cloudy, discolored, or contains particulate matter.
1.
Withdraw 20 mL (500 mg) of ZYNYZ from one vial and discard vial with any unused portion.
2.
Dilute ZYNYZ with either 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to a final concentration between 1.4 mg/mL to 10 mg/mL. Use polyvinylchloride (PVC) and di-2-ethylhexyl phthalate (DEHP), polyolefin copolymer, polyolefin with polyamide, or ethylene vinyl acetate infusion bags.
3.
Mix diluted solution by gentle inversion. Do not shake.
4.
Visually inspect the infusion bag for particulate matter and discoloration prior to administration. Discard if the solution is discolored or contains particulate matter.
Storage of diluted ZYNYZ solution
Protect the diluted ZYNYZ solution from light during storage.
Store diluted ZYNYZ solution:
At room temperature (up to 25°C [77°F]) for no more than 8 hours from the time of preparation to the end of the infusion.
OR
Under refrigeration at 2°C to 8°C (36°F to 46°F) for no more than 24 hours from the time of preparation to the end of the infusion. If refrigerated, allow the diluted solution to come to room temperature prior to administration. The diluted solution must be administered within 4 hours (including infusion time) once it is removed from the refrigerator. Do not freeze or shake diluted solution.
DO
- Administer diluted ZYNYZ solution by IV infusion over 30 minutes
- Use a polyethylene, polyurethane, or PVC with DEHP intravenous line containing a sterile, non-pyrogenic, low-protein binding polyethersulfone, polyvinylidene fluoride, or cellulose acetate 0.2 micron to 5 micron in-line or add-on filter or 15 micron mesh in-line or add-on filter
DO NOT
- Do not co-administer other drugs through the same infusion line
- Do not administer ZYNYZ as an intravenous push or bolus injection
Reference: 1. ZYNYZ Prescribing Information. Wilmington, DE: Incyte Corporation.