ZYNYZ® was studied against the previous standard of care1
The first ever completed phase 3 study of a PD-1 inhibitor in SCAC
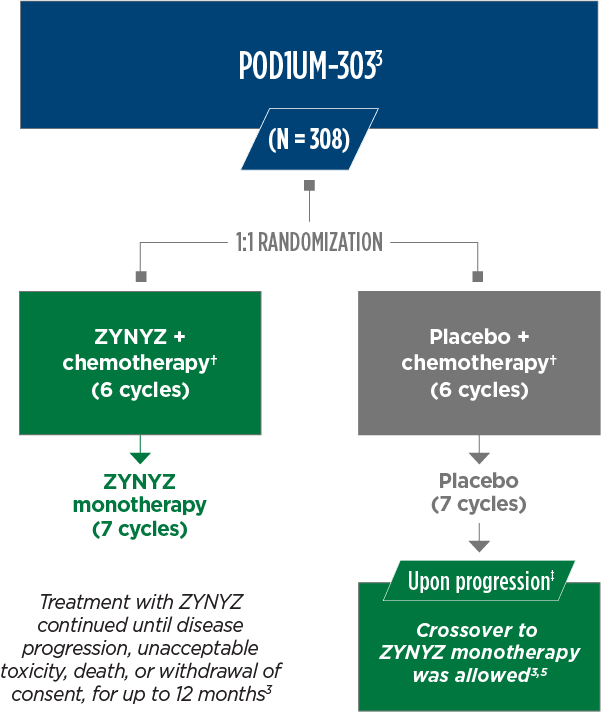
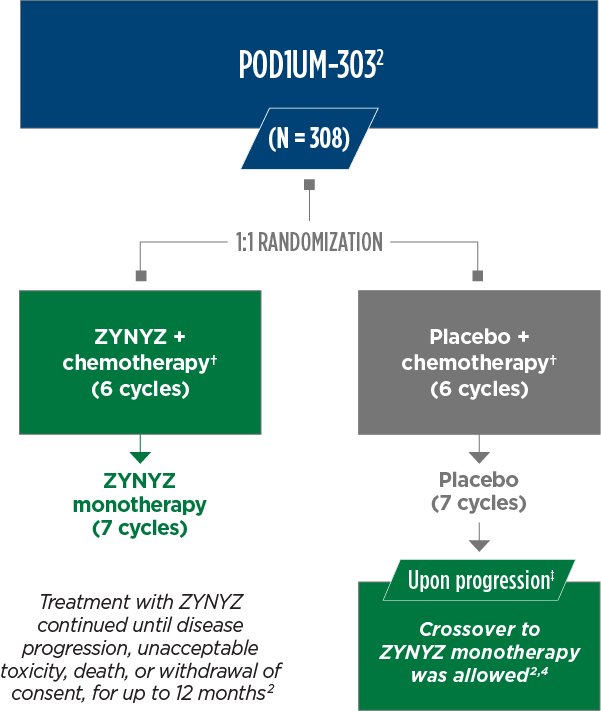
POD1UM-303/InterAACT 2 Study Design
POD1UM-303 is a randomized, multicenter, double-blind, phase 3 trial in 308 adult patients with chemotherapy-naïve inoperable locally recurrent or metastatic squamous cell carcinoma of the anal canal (SCAC) that compared ZYNYZ or placebo in combination with carboplatin/paclitaxel.2,3
SELECT ELIGIBILITY CRITERIA2
POD1UM-303 enrolled patients who had not received prior PD-(L)1–directed therapy or systemic therapy (other than a radiosensitizing agent or neoadjuvant/adjuvant therapy completed >6 months prior to study entry).
SELECT PATIENT DEMOGRAPHICS1,2
- 3.6% HIV positive
- 36% liver metastases
- 72% female
- Median age: 62 years (range: 29-86)
MAJOR EFFICACY OUTCOMES2,4
- Primary endpoint: PFS measured by BICR*
- Key secondary endpoint: OS
- Additional secondary endpoints:
- ORR, DOR, DCR, safety
Patients with well-controlled HIV were eligible to enroll in POD1UM-3032§
*Defined as the time from the date of randomization until disease progression according to RECIST v1.1 by BICR or death due to any cause.2,4
†ZYNYZ or placebo were given Q4W IV alongside chemotherapy per SOC (28-day cycle): carboplatin (AUC 5 on day 1) and paclitaxel (80 mg/m2 on days 1, 8, and 15).2,4
‡Documentation of verified radiographic progression of disease by BICR assessment.2,4
§CD4+ count ≥200 cells/μL, undetectable viral load, and receiving antiretroviral therapy.2
AUC, area under the curve; BICR, blinded independent central review; CD, cluster of differentiation; DCR, disease control rate; DOR, duration of response; HIV, human immunodeficiency virus; ORR, overall response rate; OS, overall survival; PD-(L)1, programmed death receptor (ligand)-1; PFS, progression-free survival; Q4W, every 4 weeks; RECIST, Response Evaluation Criteria in Solid Tumors; SOC, standard of care.
ZYNYZ: a paradigm-shifting PD-1 inhibitor
PROGRESSION-FREE SURVIVAL | PRIMARY ENDPOINT
HR (95% CI)*: 0.63 (0.47, 0.84); P = 0.0006†
37% reduction in the risk of disease progression or death
with ZYNYZ + carboplatin/paclitaxel vs placebo + carboplatin/paclitaxel2
PROGRESSION-FREE SURVIVAL | PRIMARY ENDPOINT
HR (95% CI)*: 0.63 (0.47, 0.84); P = 0.0006†
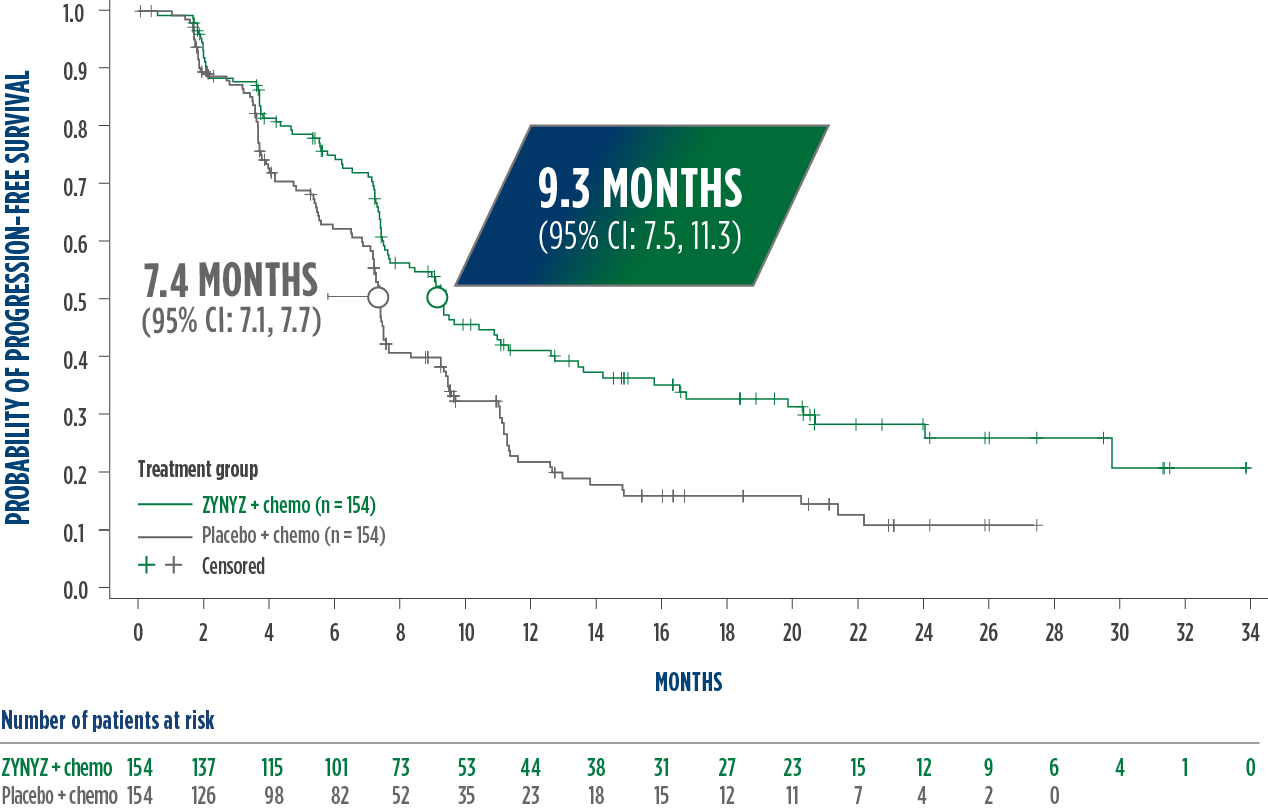
Events: 60% (n = 92) with ZYNYZ + chemotherapy vs 71% (n = 110) with placebo + chemotherapy.
*Based on stratified Cox model.
†One-sided P value based on stratified log-rank test.
CI, confidence interval; HR, hazard ratio.
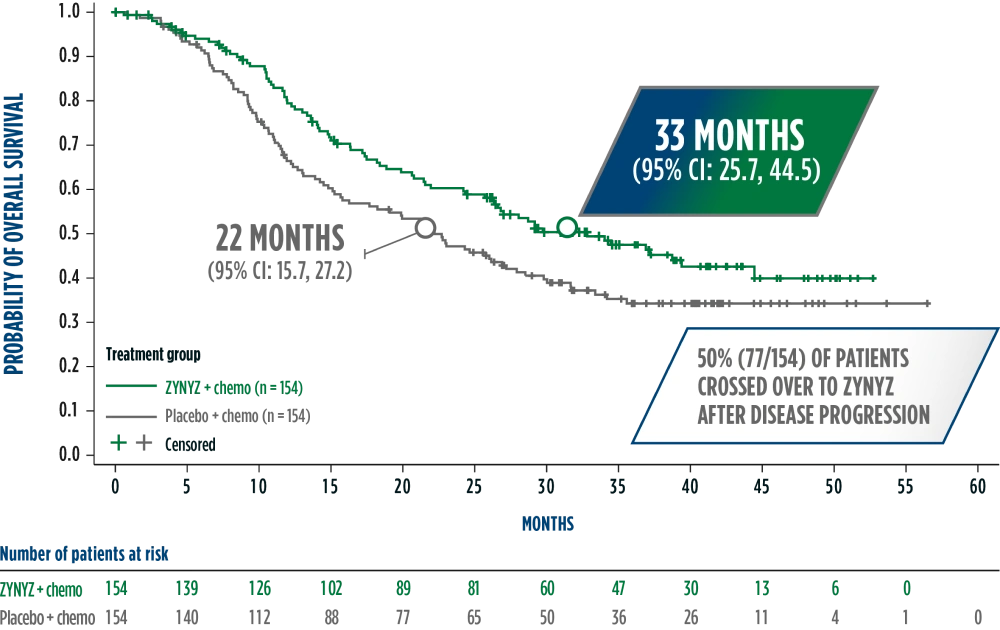
Overall survival results from POD1UM-303
HR (95% CI)‡: 0.75 (0.55, 1.01)
33 months median overall survival with ZYNYZ + chemotherapy
22 months for placebo + chemotherapy5
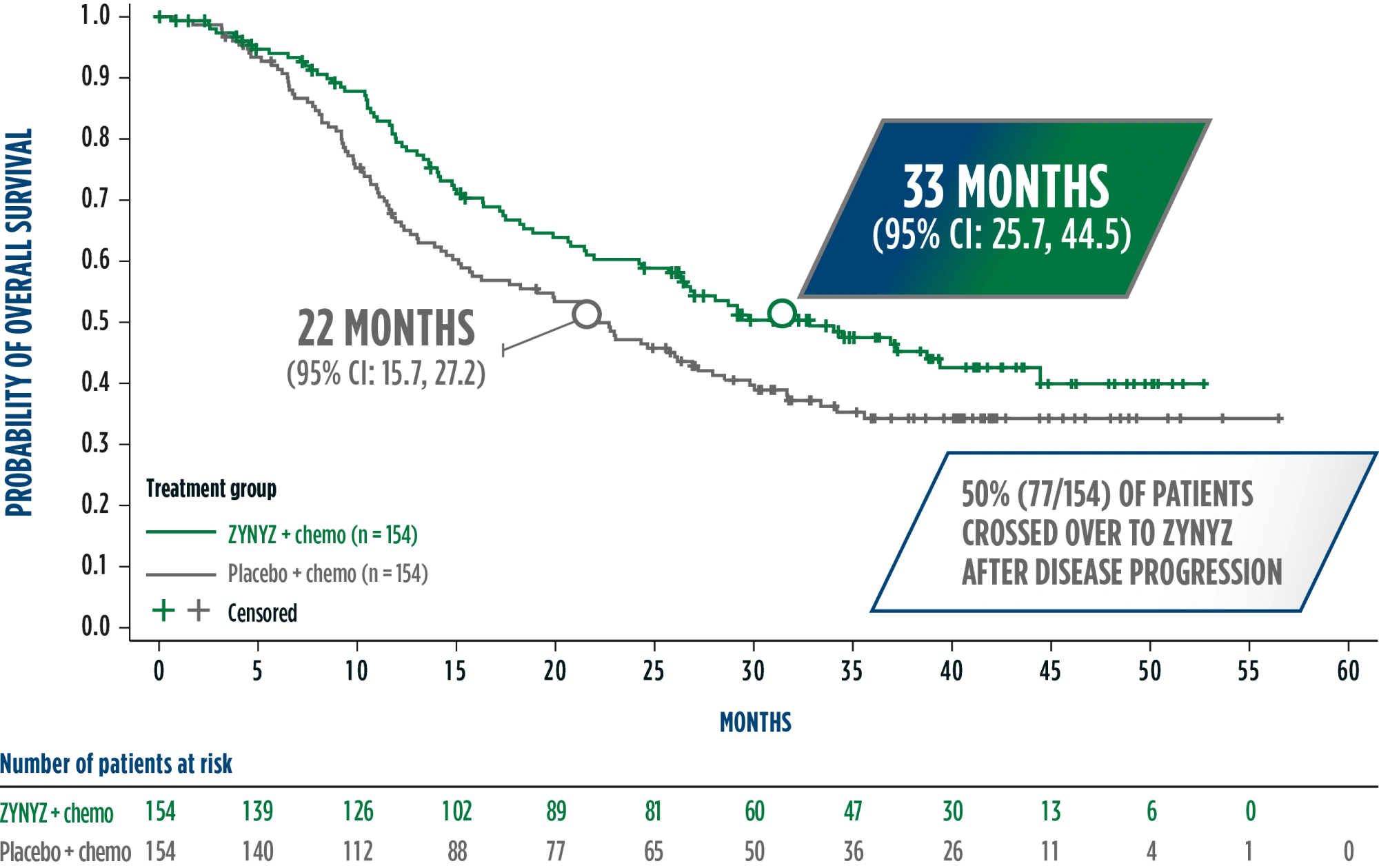
Deaths: 51% (n = 78) with ZYNYZ + chemotherapy vs 61% (n = 94) with placebo + chemotherapy.
‡Based on stratified Cox model.
- The FDA-reviewed interim analysis showed a 29-month median OS for ZYNYZ + chemotherapy (95% CI: 24.2, NE) and a 23-month median OS for placebo + chemotherapy (95% CI: 15.1, 27.9).2
LIMITATIONS:
The results of the overall survival analyses, both interim and final, did not reach statistical significance. The crossover adjustment using the RPSFT model was conducted as a post-hoc analysis. These results need cautious interpretation and could represent a chance finding.
Data from the final OS analysis are not currently included in the prescribing information.
NE, not evaluable; RPSFT, rank-preserving structural failure time.
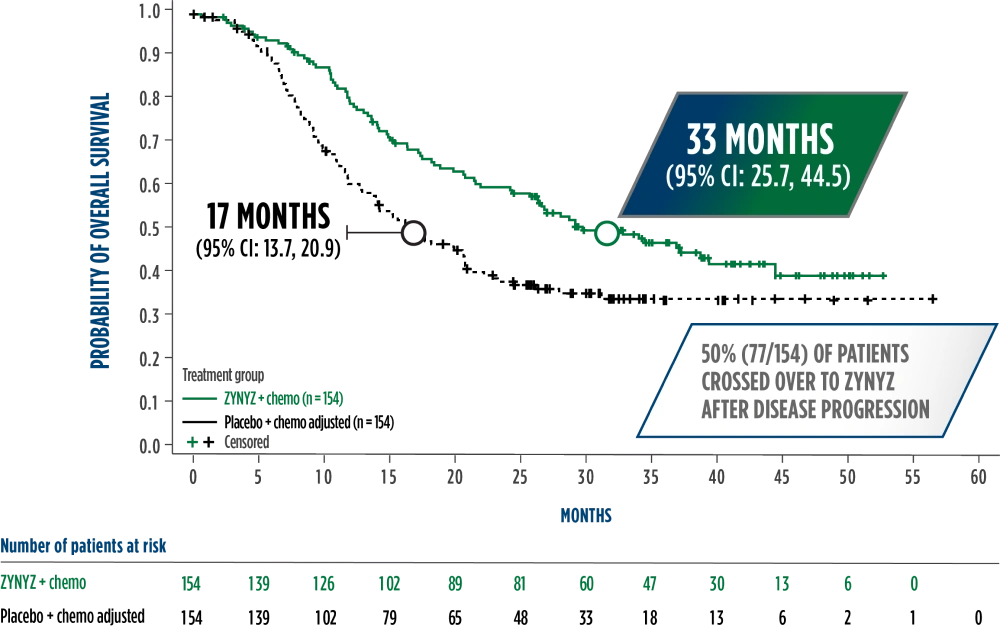
HR (95% CI)¶: 0.63 (0.47, 0.86)
After adjusting for crossover using the rank-preserving structural failure time (RPSFT) model, there was a 16-month difference in the estimated median OS in the ZYNYZ + chemotherapy group compared with the placebo + chemotherapy group5§
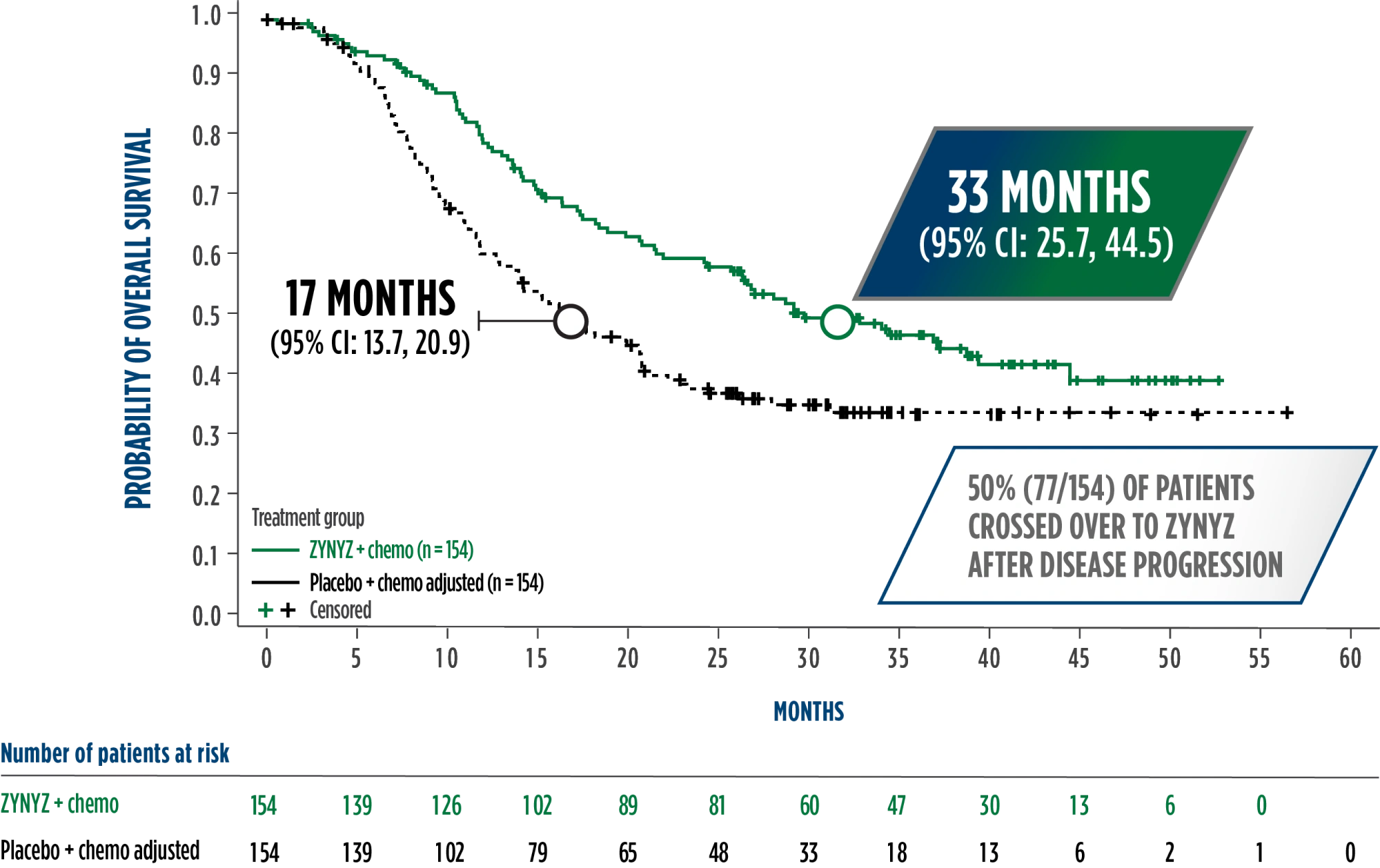
Chemotherapy regimen consisted of carboplatin/paclitaxel.
Deaths: 51% (n = 78) with ZYNYZ + chemotherapy vs 61% (n = 94) with placebo + chemotherapy.
§A statistical model known as RPSFT was used to estimate overall survival as if crossover had not occurred.
¶Based on stratified Cox model.
- The median OS from the primary analysis for the placebo + chemotherapy group was 22 months (95% CI: 15.7, 27.2)
LIMITATIONS:
The results of the overall survival analyses, both interim and final, did not reach statistical significance. The crossover adjustment using the RPSFT model was conducted as a post-hoc analysis. These results need cautious interpretation and could represent a chance finding.
Data from the final OS analysis are not currently included in the prescribing information.
Overall survival results from POD1UM-303
33 months median overall survival with ZYNYZ + chemotherapy
22 months for placebo + chemotherapy5
HR (95% CI)‡: 0.75 (0.55, 1.01)
Deaths: 51% (n = 78) with ZYNYZ + chemotherapy vs 61% (n = 94) with placebo + chemotherapy.
‡Based on stratified Cox model.
- The FDA-reviewed interim analysis showed a 29-month median OS for ZYNYZ + chemotherapy (95% CI: 24.2, NE) and a 23-month median OS for placebo + chemotherapy (95% CI: 15.1, 27.9).2
LIMITATIONS:
The results of the overall survival analyses, both interim and final, did not reach statistical significance. The crossover adjustment using the RPSFT model was conducted as a post-hoc analysis. These results need cautious interpretation and could represent a chance finding.
Data from the final OS analysis are not currently included in the prescribing information.
NE, not evaluable; RPSFT, rank-preserving structural failure time.
After adjusting for crossover using the rank-preserving structural failure time (RPSFT) model, there was a 16-month difference in the estimated median OS in the ZYNYZ + chemotherapy group compared with the placebo + chemotherapy group5§
HR (95% CI)¶: 0.63 (0.47, 0.86)
Chemotherapy regimen consisted of carboplatin/paclitaxel.
Deaths: 51% (n = 78) with ZYNYZ + chemotherapy vs 61% (n = 94) with placebo + chemotherapy.
§A statistical model known as RPSFT was used to estimate overall survival as if crossover had not occurred.5
¶Based on stratified Cox model.
- The median OS from the primary analysis for the placebo + chemotherapy group was 22 months (95% CI: 15.7, 27.2)
LIMITATIONS:
The results of the overall survival analyses, both interim and final, did not reach statistical significance. The crossover adjustment using the RPSFT model was conducted as a post-hoc analysis. These results need cautious interpretation and could represent a chance finding.
Data from the final OS analysis are not currently included in the prescribing information.
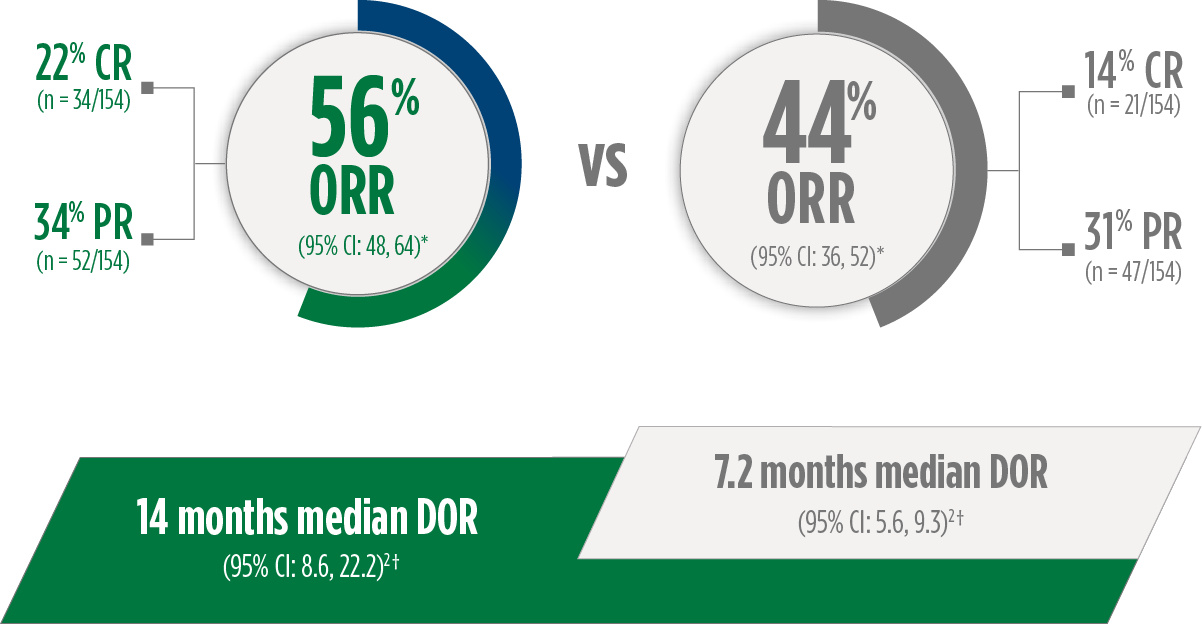
Responses with ZYNYZ® lasted ~2x as long2
ZYNYZ + CARBOPLATIN/PACLITAXEL
PLACEBO + CARBOPLATIN/PACLITAXEL
ZYNYZ + CARBOPLATIN/PACLITAXEL
PLACEBO + CARBOPLATIN/PACLITAXEL
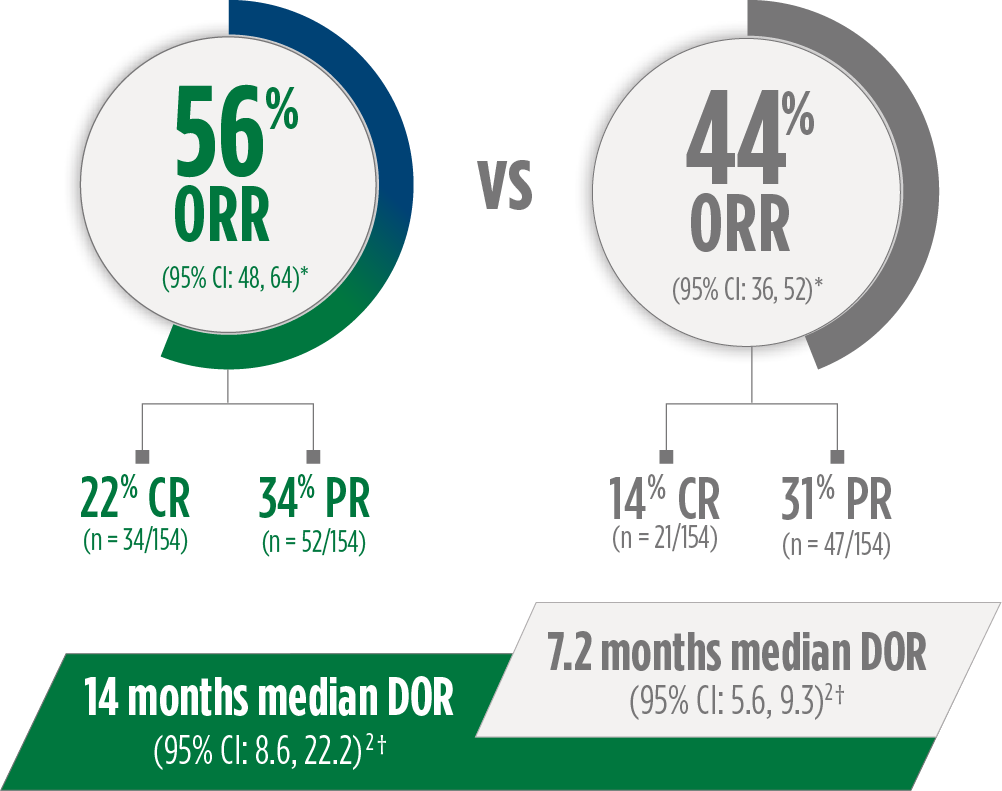
*ORR assessed by BICR.
†DOR assessed by BICR.
CR, complete response; PR, partial response.
POD1UM-202 Study Design
POD1UM-202 was an open-label, multicenter, single-arm, phase 2 study that evaluated ZYNYZ monotherapy in adult patients with locally recurrent or metastatic SCAC who progressed on or were intolerant of platinum-based chemotherapy.2,6
SELECT ELIGIBILITY CRITERIA2,6
- Inclusion criteria:
- Progression on or intolerance of platinum-based chemotherapy*
- Well-controlled HIV (if positive)†
- ECOG performance status 0-1
- Exclusion criteria:
- Prior PD-(L)1–directed therapy
- Active autoimmune disease or medical condition requiring immunosuppression
SELECT PATIENT DEMOGRAPHICS2,6
- 10% HIV positive
- 42% liver metastases
- 49% ≥65 years (range: 37-94)
- 65% female

Treatment continued until disease progression, unacceptable toxicity, or up to 24 months
*Patients who had received platinum-based therapy had received no more than 2 lines of prior systemic therapy for metastatic disease; patients who were ineligible for platinum-based therapy received at least one prior line of systemic therapy.6
†CD4+ count ≥300 cells/µL, undetectable viral load, and receiving antiretroviral therapy.2,6
‡As assessed by an independent central review committee according to RECIST v1.1.2,6
2L, second-line.

Treatment continued until disease progression, unacceptable toxicity, or up to 24 months
MAJOR EFFICACY OUTCOMES2,6‡
- Primary endpoint: ORR
- Key secondary endpoint: DOR
*Patients who had received platinum-based therapy had received no more than 2 lines of prior systemic therapy for metastatic disease; patients who were ineligible for platinum-based therapy received at least one prior line of systemic therapy.6
†CD4+ count ≥300 cells/µL, undetectable viral load, and receiving antiretroviral therapy.2
‡As assessed by an independent central review committee according to RECIST v1.1.2,6
2L, second-line.
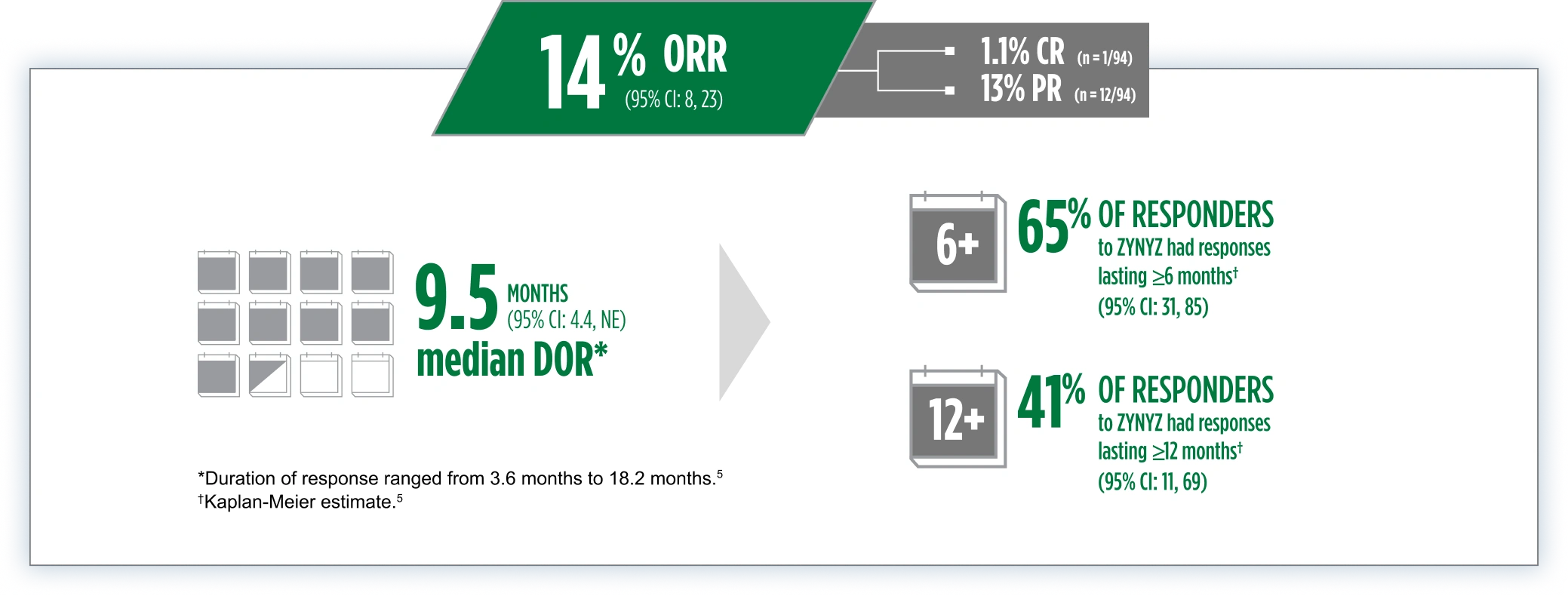
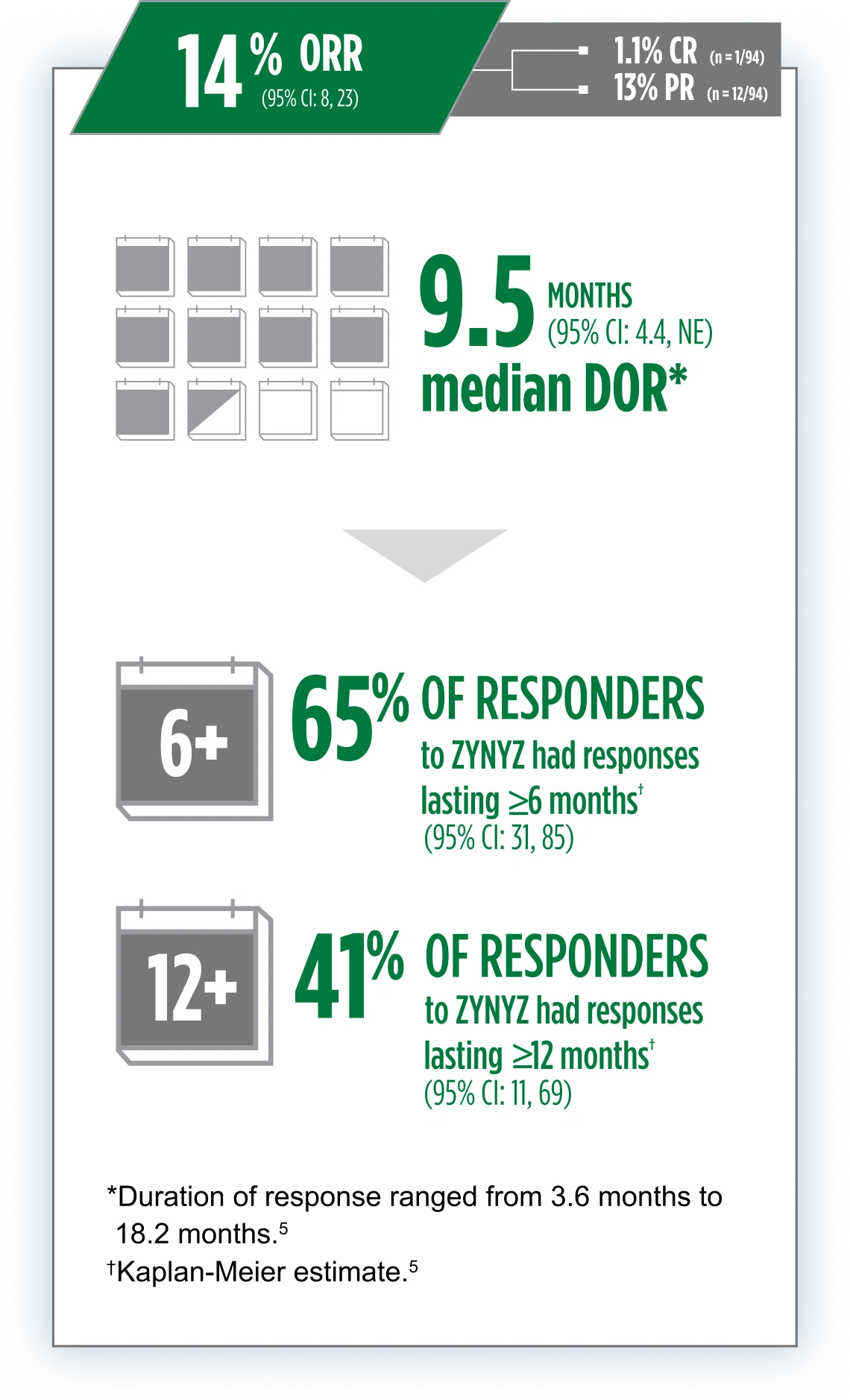
ZYNYZ monotherapy led to durable responses in 2L locally recurrent or metastatic SCAC2
References: 1. Rao S, Samalin-Scalzi E, Evesque L, et al. Retifanlimab with carboplatin and paclitaxel for locally recurrent or metastatic squamous cell carcinoma of the anal canal (POD1UM-303/InterAACT-2): a global, phase 3 randomised controlled trial. Lancet. 2025;405(10495):2144-2152. 2. ZYNYZ Prescribing Information. Wilmington, DE: Incyte Corporation. 3. Carboplatin-paclitaxel with retifanlimab or placebo in participants with locally advanced or metastatic squamous cell anal carcinoma (POD1UM-303/InterAACT 2). NIH National Library of Medicine. Accessed October 29, 2025. https://clinicaltrials.gov/ct2/show/NCT04472429. 4. Rao S, Jones M, Bowman J, Tian C, Spano JP. POD1UM-303/InterAACT 2: A phase III, global, randomized, double-blind study of retifanlimab or placebo plus carboplatin-paclitaxel in patients with locally advanced or metastatic squamous cell anal carcinoma. Front Oncol. 2022;12:935383. doi:10.3389.fonc.2022.935383. 5. Data on file. Incyte Corporation. 6. Rao S, Anandappa G, Capdevila J, et al. A phase II study of retifanlimab (INCMGA00012) in patients with squamous cell carcinoma of the anal canal who have progressed following platinum-based chemotherapy (POD1UM-202). ESMO Open. 2022;7(4):100529. doi:10.1016/j.esmoop.2022.100529.